What Is Dual Diagnosis? Why Addiction and Mental Illness Have to Be Treated Together
Dual diagnosis treatment India explained: why addiction and mental illness must be treated together, what integrated care looks like, and how to find real help.
Some struggles never come alone.
A man drinks to quiet his anxiety. A young woman uses sedatives to outrun grief. The substance is not the whole story. There is pain underneath it.
This is dual diagnosis. And it is far more common than most families realise.
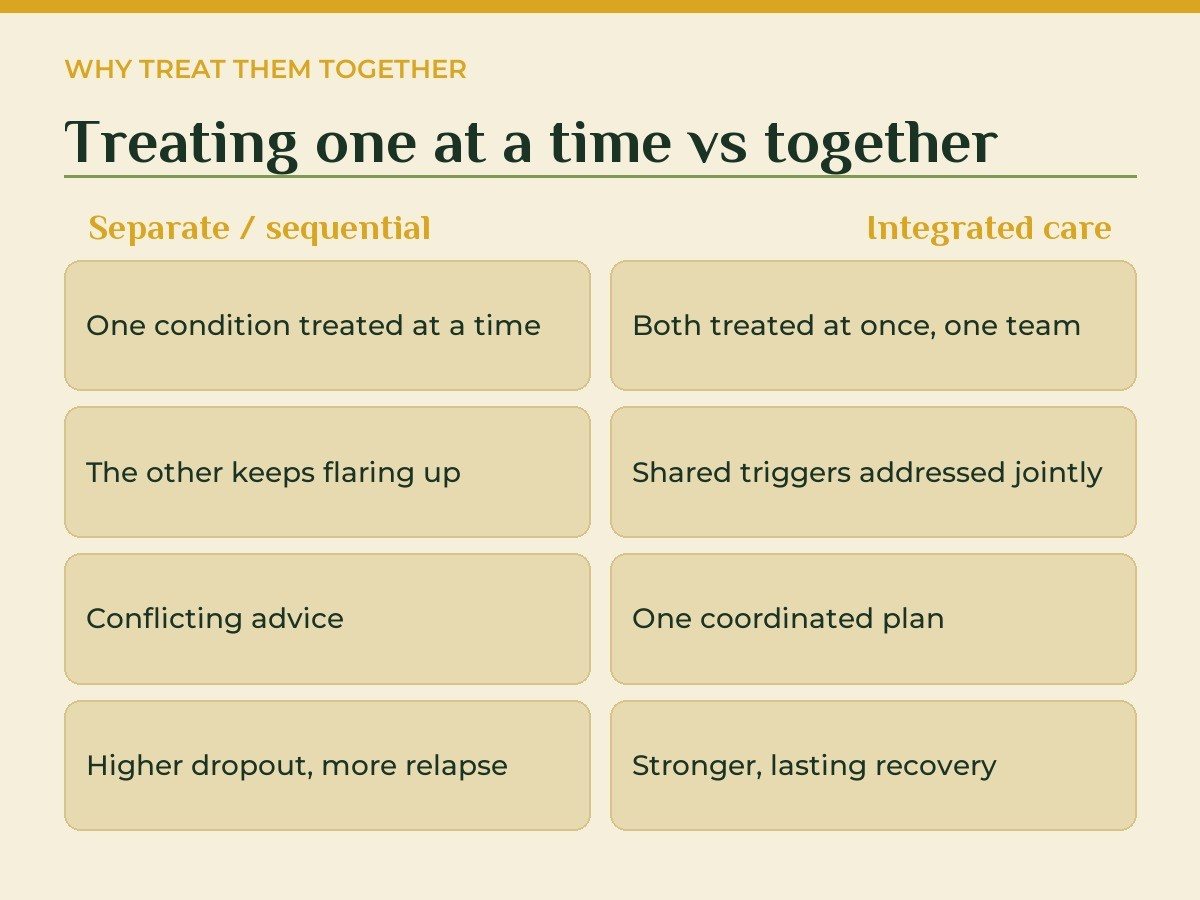
Dual diagnosis treatment in India means treating both problems at once. One team. One plan. Both the addiction and the mental illness, side by side.
When only one half gets care, the other tends to pull the person back. Treat the drinking but ignore the depression, and relapse waits quietly.
This guide explains what dual diagnosis is. Why co-occurring disorders feed each other. And what real integrated care looks like in India today.
We will keep it plain. No jargon for its own sake. Just what you need to make a good decision for someone you love.
What Does Dual Diagnosis Actually Mean?
Let us define it simply.
Dual diagnosis means two conditions in one person. A mental health condition and a substance use problem, at the same time.
Clinicians also call this co-occurring disorders. Both terms point to the same thing.
The mental health side might be depression, anxiety, bipolar disorder, or trauma. The substance side might be alcohol, cannabis, opioids, or prescription drug misuse.
Neither one caused the other in a simple line. They sit together. They shape each other.
Sometimes the mental illness comes first. A person feels low, then drinks to cope. Sometimes the substance comes first. Heavy use then triggers anxiety or low mood.
Often the order is unclear. What matters is that both are active now.
Think of it as two locked doors. Open only one, and the room stays dark. Both need a key.
This is also why labels matter less than care. A person is not "an addict" or "a depressed patient." They carry two linked conditions.
That framing changes everything. It moves blame to the side. It puts treatment at the centre.
In India, substance-linked problems are not a side issue. They were the single largest contributor to mental morbidity in the National Mental Health Survey 2015â16 (Source: NIMHANS / NMHS, 2016 â indianmhs.nimhans.ac.in).
So this overlap touches a huge number of families.
Q: Is dual diagnosis the same as co-occurring disorders?
A: Yes. Dual diagnosis and co-occurring disorders describe the same situation. A person has a mental health condition and a substance use disorder together. The two terms are used interchangeably by clinicians.
How Common Are Co-occurring Disorders in India?
This is not rare.
Indian de-addiction and psychiatric centres report co-occurring conditions in a large share of the people they see. Studies put the overlap across a wide band of patients.
The national picture backs this up. Mental and behavioural problems from substance use made up the biggest single slice of mental morbidity in the NMHS 2015â16 (Source: NIMHANS / NMHS, 2016 â indianmhs.nimhans.ac.in).
Alcohol use disorder alone is widespread. The survey found a prevalence of about 4.7%, with a sharp male skew (Source: Indian alcohol-use research review, 2024 â pmc.ncbi.nlm.nih.gov).
Now layer mental illness on top of that. The two often travel together.
Depression and drinking, for instance, frequently co-exist. Indian survey data has shown notable rates of this exact pairing (Source: NMHS / NIMHANS, 2016 â pmc.ncbi.nlm.nih.gov).
Yet most people get no care at all. India's mental health treatment gap is wide. Most adults with a condition receive no formal treatment (Source: NMHS, 2016 â healthcareexecutive.in).
That gap hits dual diagnosis hard. People fall between two systems.
Stigma plays a big part. Many families fear judgement. So they wait, or hide the problem entirely.
Access is another barrier. Trained psychiatrists are scarce in much of India. Specialist dual diagnosis care is scarcer still.
The result is delay. People reach help only in crisis. Earlier care would spare so much pain.
Q: How many people in India live with co-occurring disorders?
A: Exact national counts are limited. But Indian clinic studies and the NMHS both show substance-linked conditions are very common. The overlap with mood and anxiety disorders is well documented in treatment settings.
Why Addiction and Mental Illness Feed Each Other
Picture a loop.
Anxiety rises. A drink takes the edge off. The relief is real but short. The anxiety returns harder the next day.
So the person drinks again. The loop tightens.
This is the heart of dual diagnosis. Each condition fuels the other.
Substances can change brain chemistry over time. They can deepen depression. They can sharpen anxiety. They can trigger sleep problems and mood swings.
Mental illness pushes the other way. Low mood saps motivation. Trauma keeps the nervous system on alert. Substances become a way to cope.
Both directions are real. Both are happening at once.
There is also a shared root. Stress, trauma, genetics, and environment can drive both conditions together (Source: NIMH, 2024 â nimh.nih.gov).
The brain's reward system sits at the centre. Substances flood it with quick relief. Over time, normal pleasures feel flat.
That flatness can deepen depression. The person then leans harder on the substance. The loop turns once more.
Sleep is often the first thing to break. Broken sleep frays mood and willpower. Cravings grow sharper on tired days.
This is why treating one alone so often fails. Remove the drink, and the untreated anxiety remains. The pull comes back.
Q: Does addiction cause mental illness, or the other way around?
A: It can go either way, and often both. Sometimes mental illness comes first and substances follow. Sometimes heavy use triggers mood or anxiety problems. Shared roots like trauma and stress feed both.
Here is a hard truth.
Treating addiction alone, while ignoring the mental illness, often ends in relapse. The reverse is just as true.
Imagine detox without therapy. The body clears the substance. But the depression that drove the drinking is still there.
So the person leaves rehab feeling raw. The low mood remains. Within weeks, the old coping habit returns.
This is why integrated care matters so much. Research on dual diagnosis stresses treating both conditions together, not in separate silos (Source: Indian Journal of Psychiatry / PMC, 2018 â pmc.ncbi.nlm.nih.gov).
When care is split, things slip. The addiction clinic may not manage the psychiatric side. The psychiatrist may not track the substance use.
The person bounces between them. Messages get crossed. Medication and recovery goals clash.
Integrated treatment closes that gap. One team holds the whole picture.
Q: Why does treating only addiction fail so often?
A: Because the mental health condition stays untreated. Low mood, anxiety, or trauma keeps driving the urge to use. Without care for both, relapse risk stays high even after detox.
What Integrated Dual Diagnosis Treatment Looks Like
Good care is joined up.
Integrated treatment means one clinical team. They treat the addiction and the mental illness together, under one roof.
It usually starts with a full assessment. A psychiatrist and therapist map both conditions. They look at history, triggers, and risk.
Then comes medically supervised detox where needed. This clears the substance safely. Medical staff watch for withdrawal and mood changes.
Therapy runs alongside. Common approaches include cognitive behavioural therapy and dialectical behaviour therapy. Motivational interviewing helps build readiness to change.
Trauma-focused work is added where trauma is part of the story. This is not optional for many people.
A psychiatrist manages medication for the mental health condition. This might be an antidepressant or a mood stabiliser. Always under proper review, never guesswork.
Medication is never the whole answer. It steadies the ground. Therapy then does the deeper work.
Group sessions add another layer. People meet others on the same path. Shared stories cut through shame.
Relapse-prevention planning is built in early. The team maps triggers with the person. They rehearse what to do when cravings hit.
A typical day mixes structure and rest. There are therapy slots and group time. There is also space for sleep, exercise, and quiet.
Evidence supports this blended model. Psychosocial work plus medical care produces better dual diagnosis outcomes than fragmented treatment (Source: Indian Journal of Psychiatry / PMC, 2018 â pmc.ncbi.nlm.nih.gov).
Family work matters too. Relatives learn the condition. They learn how to support without enabling.
The goal is a tailored plan, built around the real person. Not a template.
Progress is reviewed often. The plan shifts as the person changes. Recovery is rarely a straight line.
That flexibility is the point. Good care meets people where they are. It adapts, week by week.
Small wins are tracked and named. A calmer week. A craving resisted. These build real momentum over time.
Q: What does integrated dual diagnosis care include?
A: It includes joint assessment, supervised detox where needed, and therapy like CBT and DBT. A psychiatrist manages any medication. Family support and relapse prevention complete the plan.
Conditions That Often Appear Together
Some pairings show up again and again.
Depression and alcohol use sit at the top. Many people drink to numb low mood. The drinking then deepens the depression.
Anxiety and sedative or alcohol misuse form another common pair. The substance calms the body briefly. Dependence builds quietly.
Trauma and substance use are deeply linked. Past trauma keeps the nervous system tense. Substances offer short relief, then trap the person.
Bipolar disorder and stimulant use can also overlap. Highs and lows tangle with the drug's effects. This pairing needs careful psychiatric care.
Severe conditions like schizophrenia can co-occur with cannabis or other use. Here, integrated care is vital, not a luxury.
The shared thread is simple. The substance starts as a way to cope. Over time, it becomes a second illness.
In India, alcohol leads the substance side for many adults. Its disorder prevalence is well documented across surveys (Source: Indian alcohol-use research review, 2024 â pmc.ncbi.nlm.nih.gov).
Knowing the pairing helps shape the plan. Each combination needs a slightly different approach.
Sleep problems sit across all of these. Poor sleep worsens mood and cravings alike. Good care treats sleep as part of recovery.
The same is true for shame. Many people hide their use for years. Naming the pairing gently can lift that weight.
Q: Which mental illnesses most often pair with addiction?
A: Depression, anxiety, trauma-related conditions, and bipolar disorder are common. Each can drive or worsen substance use. The pairing guides which therapies and medication are used.
How Dual Diagnosis Is Assessed and Diagnosed
Good treatment starts with a clear picture.
Assessment is the first real step. A psychiatrist and therapist sit with the person. They take a full history, gently.
They ask about substance use. How much, how often, for how long. They ask about mood, sleep, and thoughts.
They look for patterns. Did low mood come before the drinking? Or after? When are the urges strongest?
Standard screening tools support this. They help measure depression, anxiety, and substance severity. The numbers guide the plan.
One challenge is overlap. Withdrawal can mimic depression. Intoxication can look like mania. So clinicians often reassess after detox.
This is why time matters. A snapshot can mislead. A clear diagnosis sometimes takes a few weeks of observation.
Physical health is checked too. Long substance use can harm the liver, heart, and sleep. These findings shape safe care.
The team also asks about safety. Are there thoughts of self-harm? Is the home setting safe right now?
These questions are not meant to alarm. They keep the person protected. Risk shapes how care begins.
Honesty makes assessment work. The more open the person can be, the better the plan. Staff are trained to ask without judgement.
The output is a single, joined-up treatment plan. It names both conditions clearly. It sets goals for each.
Q: How is dual diagnosis diagnosed?
A: Through a full psychiatric and substance-use assessment, often with screening tools. Clinicians track history, triggers, and symptoms over time. Because withdrawal can mask mood disorders, diagnosis may be confirmed after detox.
The Role of Family in Dual Diagnosis Recovery
Recovery is rarely a solo act.
Families carry a lot. Worry, exhaustion, anger, hope. All at once. Their role in recovery is large.
First, families help with early help-seeking. Most people in India never reach care, partly due to stigma (Source: NMHS, 2016 â healthcareexecutive.in). A supportive family can break that silence.
Second, families learn the condition. They learn that relapse is part of many recoveries. Not a moral failure.
Third, they learn boundaries. How to support without rescuing. How to care without enabling use.
Good programmes teach this directly. Family therapy sessions are part of integrated care. Relatives are coached, not blamed.
There is a practical side too. Families help spot early warning signs. Sleep changes. Withdrawal from people. A return of old habits.
Catching these early can prevent a full relapse. The family becomes part of the safety net.
Recovery also asks families to heal. Living with a loved one's dual diagnosis is heavy. Support for carers matters as much as support for patients.
Guilt is common among parents and partners. Many ask what they did wrong. The honest answer is rarely simple blame.
Education replaces that guilt with action. When families understand the illness, fear drops. Calm, steady support takes its place.
Communication skills help too. Programmes teach families how to talk without conflict. They learn to listen first, then respond.
Small changes at home add up. A calmer routine. Clear, kind boundaries. A home that supports recovery, not relapse.
Q: How can family support dual diagnosis recovery?
A: By encouraging early treatment, learning the condition, and setting healthy boundaries. Family therapy helps them support without enabling. They also help spot early relapse signs and keep the person connected to care.
Finding the Right Dual Diagnosis Rehab in India
Not every centre is equipped for this.
Many rehabs treat addiction only. They are not set up for the mental illness underneath. That gap leads to revolving-door relapse.
So ask hard questions before choosing dual diagnosis rehab in India.
First, ask about the psychiatrist. Is there a full-time psychiatrist on the team? Dual diagnosis needs real medical oversight.
Second, ask about integration. Is care joined up, or run in two separate tracks? You want one team, one plan.
Third, ask about detox safety. How is medically supervised detox handled? What happens if mood worsens during it?
Fourth, ask about therapy depth. Do they offer CBT, DBT, and trauma work? Or only group talks and routine?
Fifth, ask about aftercare. Recovery does not end at discharge. There should be a clear follow-up and relapse-prevention plan.
Sixth, ask about family involvement. Will relatives be coached and included? Recovery holds better with family on board.
Cost and location matter too. Residential care is a real commitment. Ask about programme length and what is covered.
Take your time with the choice. A rushed decision can cost months later. The right fit is worth the search.
Watch for red flags too. Be wary of promised cures. Be wary of guaranteed success rates. Honest care talks about management, not magic.
The treatment gap in India is real and wide (Source: NMHS, 2016 â healthcareexecutive.in). A shortage of psychiatrists makes good centres harder to find. So these questions matter.
Q: What should I look for in a dual diagnosis rehab in India?
A: Look for a full-time psychiatrist, truly integrated care, and safe supervised detox. Check that therapy includes CBT, DBT, and trauma work. Strong aftercare and honest claims are essential.
Quick Facts: Dual Diagnosis and Mental Health in India
- Mental and behavioural problems from substance use were the single largest contributor to mental morbidity in India. â (Source: NIMHANS / NMHS, 2016 â indianmhs.nimhans.ac.in).
- Alcohol use disorder prevalence was about 4.7%, with a strong male skew. â (Source: Indian alcohol-use research review, 2024 â pmc.ncbi.nlm.nih.gov).
- Most Indian adults with a mental health condition receive no formal treatment. â (Source: NMHS, 2016 â healthcareexecutive.in).
- Depression and alcohol use disorder commonly co-occur in Indian survey data. â (Source: NMHS / NIMHANS, 2016 â pmc.ncbi.nlm.nih.gov).
- Integrated psychosocial plus medical care improves dual diagnosis outcomes. â (Source: Indian Journal of Psychiatry / PMC, 2018 â pmc.ncbi.nlm.nih.gov).
- Substance use and mental disorders share roots like trauma, stress, and genetics. â (Source: NIMH, 2024 â nimh.nih.gov).
How Ganaa Approaches Dual Diagnosis Care
At Ganaa, we treat the whole person.
We are a residential mental health and rehabilitation brand in India. We care for psychiatric conditions and substance use, including dual diagnosis.
Our model is integrated by design. A psychiatrist, therapists, and care staff work as one team. They treat the addiction and the mental illness together.
We blend modern clinical science with calm, nature-based settings. Therapies like CBT and DBT sit alongside yoga, meditation, and Ayurveda. The clinical core stays evidence-led.
Care begins with a full assessment. From there, we build a tailored plan around the real person. Not a template, and never a promise of a quick cure.
We run residential programmes over 30, 60, and 90 days, plus aftercare. Recovery is supported beyond discharge, with 24/7 support throughout.
Our residential centres span several locations. They include Ganaa Delhi I and Ganaa Delhi II in New Delhi. There is also Ganaa Gurugram in Haryana. Ganaa Goa sits in South Goa. Ganaa Greater Noida rounds out the group. The Gurugram facility includes a women-only wing.
We also run OPD clinics in Faridabad, Greater Kailash, and Greater Noida for those who do not need residential care.
Families are part of the journey here. We coach relatives to support recovery and to care for themselves too.
If someone you love is struggling, you do not have to decide alone. Speak to a Ganaa admissions counsellor, or visit ganaa.in to learn more about our programmes.
The Bottom Line on Dual Diagnosis
Addiction rarely stands alone.
So often, a mental illness sits beneath the substance use. Depression, anxiety, trauma. They feed the urge to cope.
That is why dual diagnosis treatment in India must address both at once. Treat one and ignore the other, and relapse waits.
The good news is real. Integrated care works. One team, one plan, both conditions held together.
Recovery is a process, not a single event. It asks for therapy, medical care, family support, and time.
If this describes someone you love, take the next small step. Ask the hard questions. Find a centre with real psychiatric depth.
Help exists. People do get better. With the right care, a steadier life is within reach.
You do not have to carry this alone.
FAQ
Q: What is dual diagnosis treatment in India? A: Dual diagnosis treatment in India is integrated care for two conditions at once. It treats a substance use problem and a mental health condition together. One clinical team handles both. The aim is to address shared triggers and root causes, not just one half of the picture.
Q: What are co-occurring disorders? A: Co-occurring disorders means a mental health condition and a substance use disorder appear together in the same person. Common pairs include depression with alcohol use, or anxiety with sedative misuse. Each condition can feed the other, which is why both need care.
Q: Why must addiction and mental illness be treated together? A: When only one condition is treated, the other often pulls the person back. Untreated depression or anxiety can drive a return to substances. Treating addiction and mental illness together lowers this risk and supports steadier recovery.
Q: How common is dual diagnosis in India? A: Indian de-addiction and psychiatric studies report co-occurring conditions in a wide share of patients. Mental and behavioural problems from substance use were the single largest contributor to mental morbidity in the National Mental Health Survey. So the overlap is far from rare.
Q: What therapies are used in dual diagnosis rehab in India? A: Common approaches include CBT, DBT, and motivational interviewing, plus trauma-focused work where needed. A psychiatrist manages medication for the mental health condition. Family sessions and relapse-prevention planning round out the care.
Q: Can dual diagnosis be cured? A: Dual diagnosis is usually managed rather than cured outright. Many people reach long, stable recovery with the right care and ongoing support. Honest programmes talk about management and relapse prevention, not guaranteed cures.
Q: How do I choose a dual diagnosis rehab in India? A: Look for a centre with a full-time psychiatrist and integrated, not parallel, care. Ask how they handle detox, medication, and aftercare. A good programme will also involve your family and plan for life after discharge.